Objective: The aim of this study is to present the case of a 41-year-old asymptomatic male endurance athlete who underwent a competitive sports preparticipation screening examination, which revealed the presence of a huge thoracic vascular malformation with multiple fistulous communications between coronary arteries, bronchial arteries, and the pulmonary artery.
Coronary artery-pulmonary artery fistulas (CAFs) are rare cardiac anomalies. Most of them originate from the right coronary artery (RCA), while fistulas originating from the left anterior descending artery (LAD) or multiple arteries are less common. CAFs are often asymptomatic and are found incidentally during routine cardiac imaging. With this short paper, the author presents the case of a 41-year-old asymptomatic male endurance athlete who underwent a competitive sports preparticipation screening examination, which revealed the presence of a huge thoracic vascular malformation with multiple fistulous communications between coronary arteries, bronchial arteries, and the pulmonary artery.
Coronary to Pulmonary Artery Fistula; 2D TT Echocardiography; Cardiac Computed Tomography; Athlete
Coronary artery-pulmonary artery fistulas (CAFs) are rare cardiac anomalies. [1-6] Most of them originate from the right coronary artery (RCA), while fistulas originating from the left anterior descending artery (LAD) or multiple arteries are less common [1]. CAFs are often asymptomatic and are found incidentally during routine cardiac imaging in athetes underwent sports preparticipation screening [2-3-4-5].
Arteriovenous fistula is a rare form of congenital heart disease, which can also occur in asymptomatic athletes, being an uncommon but, alas, often unrecognised type of congenital coronary anomaly. An arterial fistula is an abnormal conduit between arteries in communication with each other and therefore does not alter haemodynamics, as intracardiac and systemic pressures remain unchanged. In fact, when it is present between the coronary artery and the cardiac chambers, we speak of a coronary-chamber fistula; furthermore, the fistula may also be present between a coronary artery and another arterial vessel adjacent to the pulmonary or systemic circulation [2-6]. With this short paper, the author presents the case of a 41-year-old asymptomatic male endurance athlete who underwent a competitive sports preparticipation screening examination, which revealed the presence of a huge thoracic vascular malformation with multiple fistulous communications between coronary arteries, bronchial arteries, and the pulmonary artery.
Here, a 41 year-old asymptomatic athlete underwent preparticipation sports screening. To sum up, before the routine ECG screening, there was an intermittent postero-septal accessory pathway with left ventricular pre-excitation without symptoms or other abnormalities. This ECG anomaly disappeared during the Exercise-ECG stress test. Physical examination was normal and the family history was unremarkable for heart disease. The athlete underwent two-dimensional trans-thoracic echocardiography (2DTTE) to rule out underlying cardiac disease. However, Color-Doppler examination from parasternal short axis view (PSAX) showed an anomalous diastolic jet directed into the main pulmonary artery trunk (Figure. 1). A coronary artery fistula was suspected even though left-to-right shunt was not significant and there were no signs of pulmonary or systemic flow overload. Subsequent cardiac computed tomography (CCT) was performed and it showed a complex fistula originating from all proximal coronaries and draining into the main pulmonary artery. In particular, CCT showed a large vascular malformation (Figure. 2) constituted by multiple fistulous communications between coronary arteries, bronchial arteries, and the pulmonary artery. Coronary angiography showed the presence of numerous fistulas with coronary-pulmonary Left to Right (coronary to pulmonary) moderate shunt as well as another communication between the descending aorta and a branch of the pulmonary artery with patent epicardial coronary arteries. In view of the lack of symptoms and signs of left ventricular overload, the athlete was considered eligible for competitive sport, but, by consensus opinion, he must be monitored with ECG stress test plus echocardiography every 6 months.
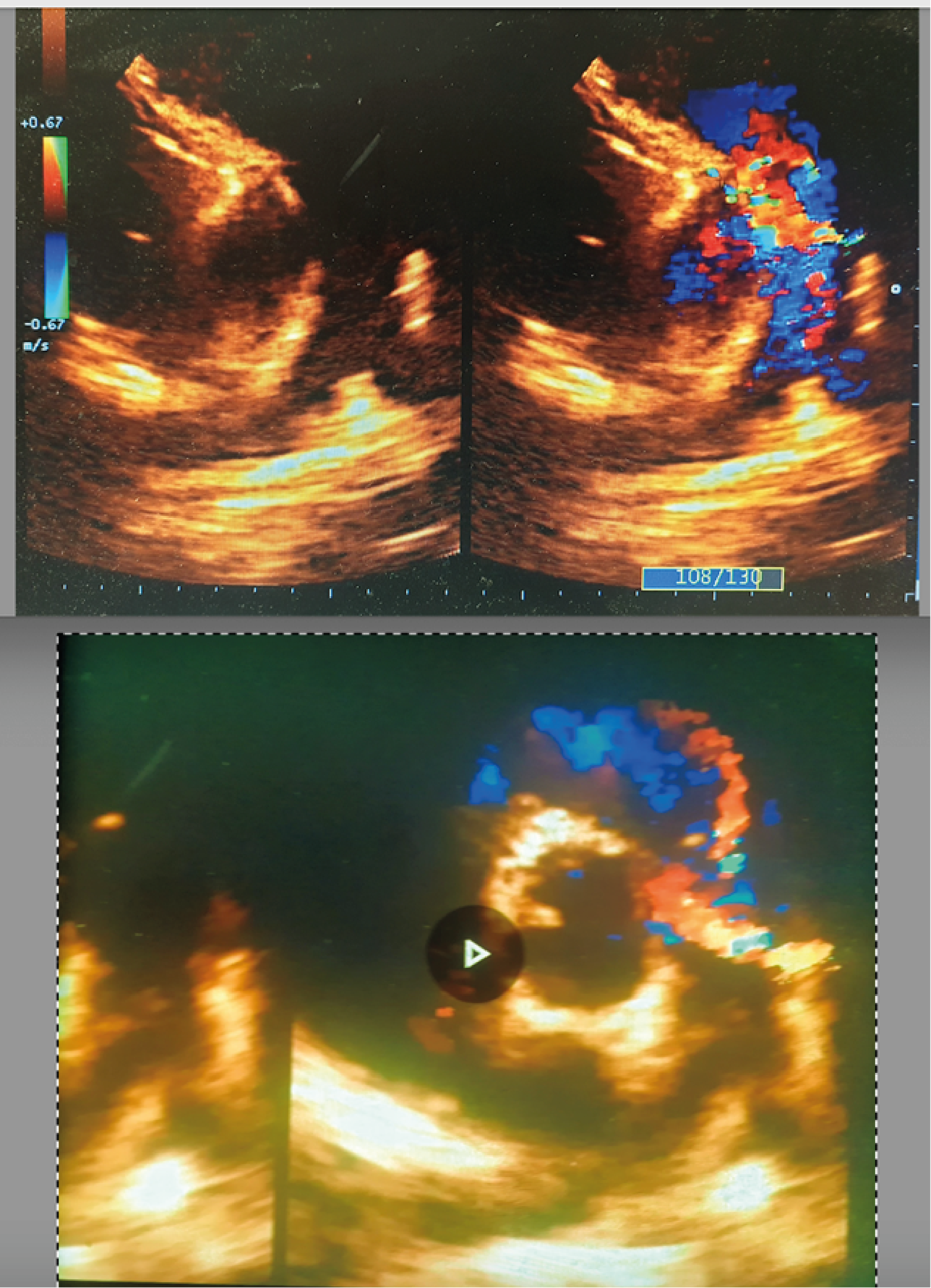
Figure 1: 2D TT echocardiography showing the jet of the fistula between coronary artery and pulmonary artery from the magnified PSAX view.
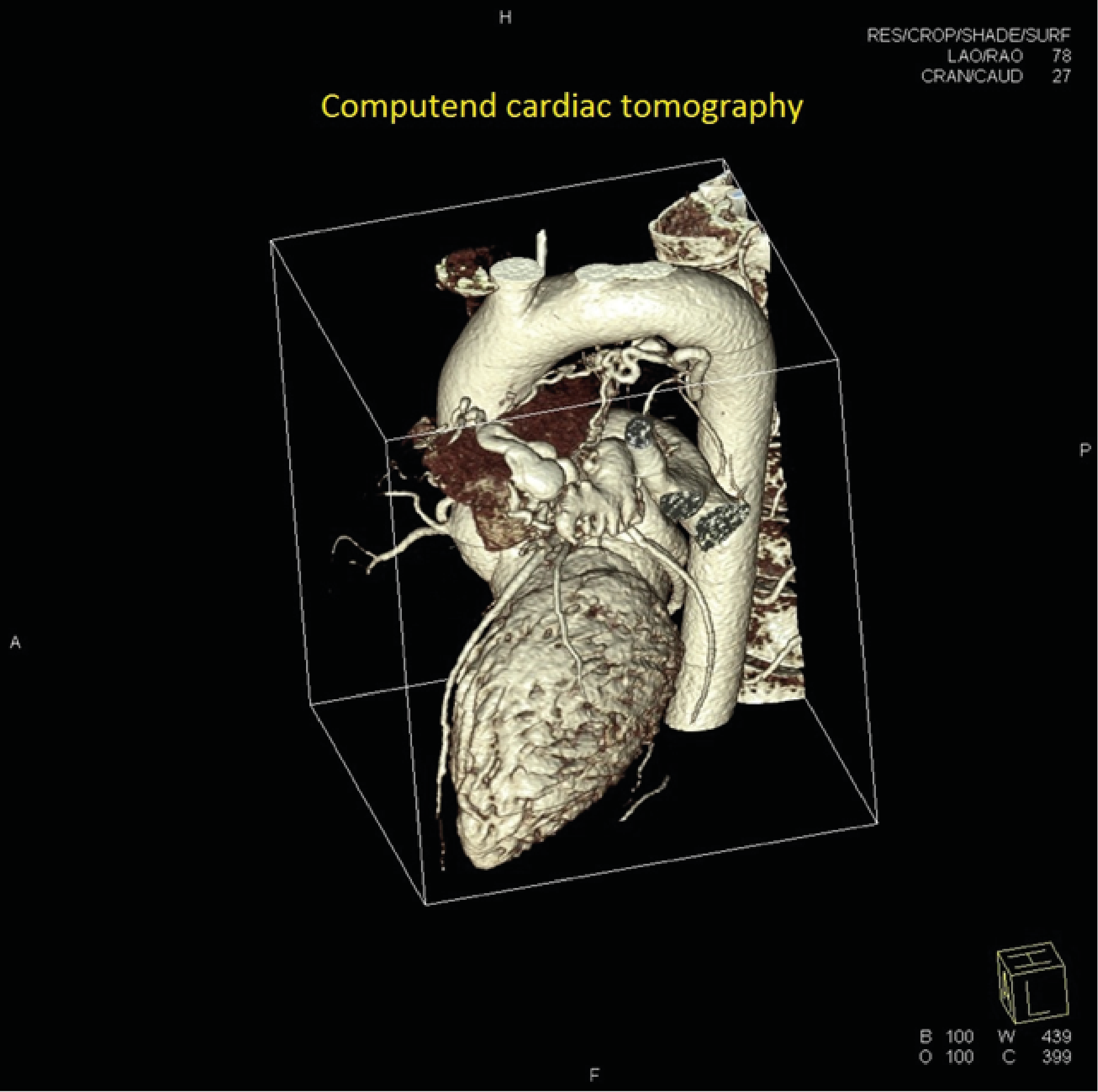
Figure 2: Computed Cardiac Tomography showed a large vascular malformation in the chest.
Coronary fistulas are an uncommon coronary artery abnormality but still present even in asymptomatic subjects, like athletes. This clinical case highlights the usefulness of sports preparticipation screening in athletes and cardiac imaging diagnostics through color Doppler echocardiography plus cardiac computed tomography.
- Ufuk F, Kılıç O, Kılıç ID (2020) Anomalous origin of the right coronary artery from the pulmonary artery and simultaneous coronary-bronchial artery fistula. Anatol J Cardiol. 23: E10-E1 [Crossref]
- Abhyankar AD, Mok NS, Helprin GA, Pressley L (1996) Multiple coronary-pulmonary fistulae involving all three coronary arteries: a case report .Int J Cardiol 57 :181-183. [Crossref]
- Maron BJ, Doerer JJ, Haas TS, et al (2009) Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States. Circulation 119: 1085-1092. [Crossref]
- Mont L, Pelliccia A, Sharma S, et al (2017) Pre-participation cardiovascular evaluation for athletic participants to prevent sudden death: Position paper from the EHRA and the EACPR, branches of the ESC. Eur J Prev Cardiol 24: 41–69. [Crossref]
- Corrado D, Basso C, Schiavon M, et al (2008) Pre-participation screening of young competitive athletes for prevention of sudden cardiac death. J Am Coll Cardiol 52: 1981–1989. [Crossref]
- Lytrivi ID, Wong AH, Ko HH, et al (2008) Echocardiographic diagnosis of clinically silent congenital coronary artery anomalies. Int J Cardiol 126: 386–393. [Crossref]