Metformin is an oral antidiabetic used in the treatment of type 2 diabetes mellitus. More precisely, it belongs to the class of biguanides; Metformin is used in the treatment of type 2 diabetes mellitus both as monotherapy and in combination therapy with other oral antidiabetic agents or with insulin, when dietary interventions and exercise are not sufficient to control the disease.
When used in overweight diabetic patients, metformin also causes a decrease in the complications of diabetes and its use has been associated with stabilization and, albeit modest, loss of body weight. In type 2 diabetes mellitus (called also DM2 and in the past 'adult diabetes' or 'food') the insulin produced by the pancreas is unable to fully exert its action so that the body even produces it in excess, with the result on the one hand of making increasing weight and on the other hand progressively depleting the pancreas, is unable to meet the body's needs. It is as if the body were resisting the action of insulin. Metformin reduces insulin resistance. It is taken by mouth and is the only drug useful in all stages of type 2 diabetes. It also helps improve the balance of fats and, to a limited extent, blood pressure.
Metformin alone has important effects on blood sugar. Accompanied by physical exercise, weight loss and possibly other medications, it is often an effective therapy. It does not cause hypoglycaemia, helps not to gain weight or even reduces it. The main feature of Metformin is to interact strongly with AMPK by regulating its expression. In fact, it’s down regulation leads to consuming ATP, synthesizing cholesterol and fatty acids and consuming glucose: a situation in which insulin levels are quite high (therefore energy abundance). On the contrary, it’s up regulation leads to the creation of ATP, consuming more fatty acids for energy purposes and it is a metabolic situation similar to caloric restriction in which insulin levels are kept low (therefore energy scarcity).
Metformin by up regulating AMPK has therefore shown to have a somewhat transversal therapeutic use in the treatment of metabolic dysfunctions.
Exercise; Nutritional Biochemistry; Metformin; Body Building; Inflammation; Skeletal Muscle
The use of anabolic androgenic steroids (AAS) in bodybuilding became a huge problem and risky factor that causes the death of many athletes, extreme ways are followed in bodybuilding especially during contest preparation and the goal is to get the perfect physique on stage, our goal is to help and save lives by providing scientific evidence to help the athletes and save their lives by preventing them the abuse of such drugs, in our case report series we used Metformin. Within the cell, Metformin inhibits the inflammatory pathway and activates AMPK (thereby increasing mTOR inhibition), while also modulating oxidative stress. These processes jointly affect inflammation, cellular survival, stress defense, autophagy, and protein synthesis. Metformin can increase insulin sensitivity and lower blood levels of insulin due to its ability to cleanse the microbiome, also inhibiting glucose formation in the liver, can also inhibit the release of pro-inflammatory cytokines, reduces or eliminates inflammatory factors. Metformin increases the formation of mucin-degrading Akkermansia miciniphila in the gut. Akkermansia muciniphila reduces inflammation, lowers insulin resistance so by this we can say simply that metformin boost the growth of good bacteria.
Metformin is effective and efficient drug for our case report series, because of the following mechanisms of action:
Insulin & Inflammation Suppression
Neuroprotection
Anti-Cancer Agent
Microbiome Cleansing
Akkermansia Producing
Body Fat Burning
It is interesting to note that relatively recent studies suggest that Metformin can directly inhibit the action of leucine on mTOR. Not only would this be a bad sign for muscle growth, but the inhibitory effect of Metformin on mTOR should have a major effect as it correlates with the reduction in the risk of fatal cancers in diabetics. Interesting as postulated by Dr. Melnik of the University of Osnabrück in Germany: Metformin may be a direct competitor of leucine for the binding and activity of mTORC1. The doctor noted in his article that the usual daily dose in diabetics of Metformin (2 g) is in the range of the 2 g of leucine derived from the daily consumption of 100 g of meat or cheese. Since the two substances are similar in structure and size, they can compete for the same sites in the activation of mTOR.
However, Metformin has these three characteristics of relevant interest:
Schematic representation of Gluconeogenesis
1. Increases the number and sensitivity of cell receptors for Insulin
2. Decreases the amount of glucose / sugar absorbed by the intestine
3. It decreases the amount of glucose / sugar produced by the liver (a primary source for the production of hepatic glucose is amino acids).
These three effects explain why clinical administration of Metformin rarely results in cases of greater hypoglycemic effects when administering the drug alone. However, when given in combination with insulin and / or sulfonylureas (Glipizide) injections there is a significant increase in carbohydrate requirements and weight gain.
The aforementioned characteristics expressed by Metformin have meant that this drug enters the arsenal of sports pharmacological supplementation, especially in Body Building.
Generally Body Builders use the effects of Metformin differently for different phases:
1. During the Bulk phases, with the use of exogenous insulin, 500-800mg of Metformin 1-2 times a day increased the effectiveness of the insulin. This was due to an increase in the number and sensitivity of the receptor sites. Metformin also decreases the amount of insulin required for maximum results.
2. During pancreatic regeneration or protocols containing Glipizide, Glyburide or other pancreatic stimulants / insulin, Metformin increases its effectiveness and amplifies the results. The common dose of Metformin for this purpose is 500mg 2 times a day.
3. During the Cut phases, Body Builders use Metformin as a means of decreasing the production of glucose by the liver and the absorption of glucose by the intestine. By itself, this decreases the secretion of insulin by the pancreas and increases the body's dependence on fat stores for energy needs. This is especially done while using GH and PGF-2 and creates a synergistic effect with AAS. As the cellular receptor sites for insulin are more sensitive and since there is cross stimulation between IGF-1 and insulin (and their opposite receptor sites) the retention of lean mass increases contained. This effect favors the reduction of the negative effects that a weight loss diet exerts on the endogenous production of IGF-1: if a co-administration of IGF-1 and Metformin occurs, the advantage reflects on the lower dose (of IGF-1) required and on the better receptor efficiency. .
It is known that during a calorie-deficient diet the IGF-1 produced decreases, and is one of the factors by which the stored lean mass is reduced. If the cell sites are more numerous and sensitive, stimulation requires less IGF-1. Typically, 500mg of Metformin per day is considered sufficient.
Metformin should be taken with meals and never less than six hours before going to bed. People with kidney problems should not take Metformin and most athletes should be aware that in some cases the combination with 17-alpha-alkylated drugs can induce even greater liver damage.
Design, Setting, Partecipants
The purpose of this case report series is to evaluate the potential interaction between metformin and exercise during contest prep in order to help in different contest protocols to minimize the use of extreme ways used during preparations, and save the health of bodybuilders.
The method used to measure cortisol levels: The cobas e 411 fully automated, system for immunoassay analysis
Table 1:
We increased the essential amino acids intake and GH doses (for AAS users) during the last two weeks, and every bodybuilder ingested 7g of glutamine during working out.
During contest prep the most important thing is to get the best look lean and dry BUT without putting the athlete’s life on risk of any health issues.
The key thing of this experiment was to not mess with minerals balance in the body, we know certain anabolic steroids cause minerals imbalance so we focused on that and tried using metformin during the prep and we collected blood samples from the participants every week.
The other thing i focused on was cortisol levels and inflammatory biomarkers and metformin have a direct anti-inflammatory action. Studies have suggested that metformin suppresses inflammatory response by inhibition of nuclear factor κB (NFκB) via AMP-activated protein kinase (AMPK)-dependent and independent pathways.
We noticed an improve in gut health and no digestion issue (no bloating) and was just one case had diarhea.
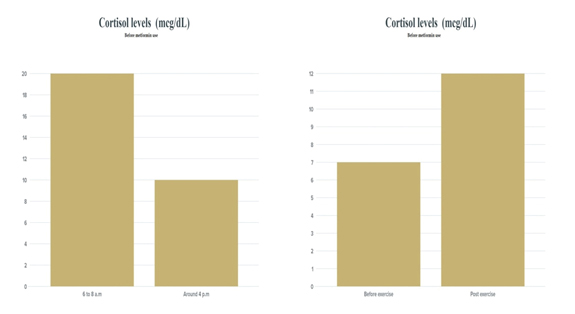
Figure 1. Cortisol levels before the use of Metformin. The data were collected a week before the experiment daily
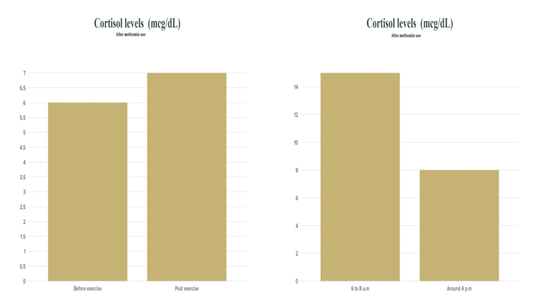
Figure 2. Cortisol levels after the use of Metformin
Therefore Metformin (by upregulating AMPK) implements:
- reduction of insulin secretion
- reduction of the synthesis of fatty acids and cholesterol from the two previous situations derives:
- increased lipolysis
- increased lipid oxidation, uptake of glucose and glycolysis in skeletal muscles
- increase in lipid oxidation and uptake of glucose by the heart
- inhibition of pro-inflammatory processes
- reduction of glucose absorption from the gastrointestinal tract to about half
- inhibition of hepatic gluconeogenesis by 36%
- increase in the number and sensitivity of insulin receptors,
- increasing the uptake of glucose on peripheral structures
- increases lipid oxidation for energy purposes
From the following meta-analysis it was found that metformin reduced by:
- 5.3% the BMI and triglycerides
- 4.5% fasting blood sugar
- 14.4% fasting insulin
- 5.6% LDL cholesterol
- 40% the onset of diabetes (in pre-diabetic subjects)
increasing HDL cholesterol by 5%. Therefore, metformin could also be used in dyslipidemic subjects with moderately altered LDL values, instead of using statins, and in association with repaglinide as it has shown on the one hand to increase insulin sensitivity and on the other to improve the lipid profile.
However, the mechanism by which it manages to activate AMPK is currently unclear, but other hypotheses on how Metformin can inhibit the hepatic production of glucose have been advanced. For example, it has been hypothesized that metformin may inhibit mitochondrial glycerol 3-phosphate dehydrogenase (mGPD) which would reduce the production of hepatic glucose from glycerol and lactate, but the shuttle system of glycerol phosphate is of little relevance.
Hepatic unlike that of aspartate malate, so much so that on an animal model the destruction of the shuttle glycerol phosphate did not alter glycaemia and it could also be expected that gluconeogenesis from lactate would not be affected since the NADH produced by the conversion of lactate pyruvate would have been consumed by 3-phosphate glyceraldehyde
dehydrogenase during gluconeogenesis.
However, a link was found between these two mechanisms, as it was found that the upregulation of AMPK inhibited mGPD in yeasts (very similar to that of humans), this would explain the possible interaction between the pathway that regulates mGPD and the direct action that Metformin exerts on AMPK.
Metformin one of the most studied drugs, based on the collected data, we found it’s suitable for our case report series, because of its anti-aging and anti-inflammatory properties, it helped the athletes to benefit and minimize the risks, and our main goal is to save many lives possible.
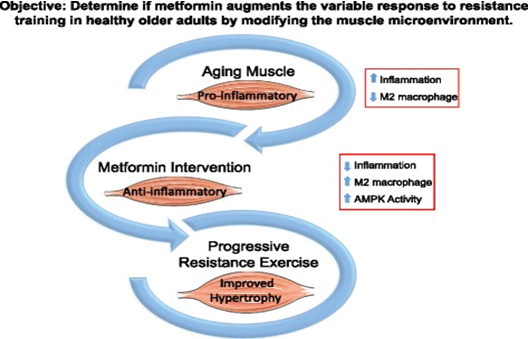
Figure 3. Objective: Determine if metformin augments the variable response to resistance training in health older adults by modifying the muscle microenvironment
Something similar might be going on with metformin and exercise. ROS, cytokines, and myokines, for example, are involved in the adaptation process. If metformin is blunting these signals, it’s interfering with the adaptation. The perceived stress in the body may be artificially attenuated by the drug and therefore the compensatory response is, too. I will save you from all of the gory details in this email, but I may elaborate on the mechanisms and biochemistry down the road.
So, if you’re a relatively healthy person that exercises regularly and takes metformin as an anti-aging drug, should you continue taking metformin? I don’t think there’s a black and white answer at this point and it depends on how you personally respond. In the most recent study, there was a high amount of variability in the metformin group in their response to exercise-induced adaptations. For me, in response to these papers, along with my personal experience of seeing slightly higher lactate levels during zone 2 training (suggesting, perhaps, less mitochondrial efficiency), I’ve reduced my dose of metformin and only take it in the evening in an effort to reduce the amount of metformin in my system when I’m awake and exercising.
Maybe there’s an optimal dosing, timing, and scheduling of metformin, fasting, nutritional makeup, and exercise that’s superior to placebo. Maybe not and it depends on your makeup and your individual response.
- Fournier (2014) Metformin and low levels of thyroid-stimulating hormone in patients with type 2 diabetes mellitus. CMAJ 186: 1138-1145. [Crossref]
- Karimifar (2014) Effect of metformin on thyroid stimulating hormone and thyroid volume in patients with prediabetes: A randomized placebo-controlled clinical trial. J Res Med Sci. 19: 1019-1026. [Crossref]
- Cappelli (2012) Thyreotropin levels in diabetic patients on metformin treatment. Eur J Endocrinol 167: 261-265. [Crossref]
- Cappelli (2009) TSH-lowering effect of metformin in type 2 diabetic patients: differences between euthyroid, untreated hypothyroid, and euthyroid on L-T4 therapy patients. Diabetes Care 32: 1589-1590. [Crossref]
- Seung YL, Chin HS, Yuan BX, et al. (2014) SMILE up regulated by metformin inhibits the function of androgen receptor in prostate cancer cells. Cancer Lett 354: 390-397. [Crossref]
- Carlo Campagnoli, Franco Berrino, Elisabetta Venturelli, et al. (2013) Metformin decreases circulating androgen and estrogen levels in nondiabetic women with breast cancer. Clin Breast Cancer 13(6):433-8. [Crossref]
- Luo T, Nocon A, Fry J (2016) AMPK Activation by metformin Suppresses Abnormal Extracellular Matrix Remodeling in Adipose Tissue and Ameliorates Insulin Resistance in Obesity. Diabetes 65: 2295-2310. [Crossref]
- Trolle B, Flyvbjerg A (2007) Efficacy of metformin in obese and non-obese women with polycystic ovary syndrome: a randomized, double-blinded, placebo-controlled cross-over trial. Hum Reprod 22: 2967-2973. [Crossref]
- Wang M, Tong JH, Zhu G (2012) Metformin for treatment of anti-psychotic-induced weight gain: a randomized, placebo-controlled study. Schizophr Res 138: 54-57. [Crossref]
- Wu RR, Jin H, Gao K (2012) Metformin for treatment of antipsychotic-induced amenorrhea and weight gain in women with first-episode schizophrenia: a double-blind, randomized, placebo-controlled study. Am J Psychiatry 169: 813-821. [Crossref]
- Chen CH, Huang MC, Kao Cf (2013) Effects of adjunctive metformin on metabolic traits in nondiabetic clozapine-treated patients with schizophrenia and the effect of metformin discontinuation on body weight: a 24-week, randomized, double-blind, placebo-controlled study. J Clin Psychiatry 74: 424-430. [Crossref]
- Peng PJ, Ho PS, Tsai CK (2016) A Pilot Study of Randomized, Head-to-Head of Meteformin Versus Topiramate in Obese People With Schizophrenia. Clin Neuropharmacol 39: 306-310. [Crossref]
- Komossa K, Depping AM, Gaudchau A (2010) Second-generation antipsychotics for major depressive disorder and dysthymia. Cochrane Database Syst Rev12:CD008121. [Crossref]
- Mogul H, Freeman R, Nguyen K (2016) Metformin-Sustained Weight Loss and Reduced Android Fat Tissue at 12 Months in Empowir (Enhance the Metabolic Profile of Women with Insulin Resistance): A Double Blind, Placebo-Controlled, Randomized Trial of Normoglycemic Women with Midlife Weight Gain. Endocr Pract 22: 575-586. [Crossref]
- van der Aa, Elst MA, van de Garde EM (2016) Long-term treatment with metformin in obese, insulin-resistant adolescents: results of a randomized double-blinded placebo-controlled trial. Nutr Diabetes 6: e228. [Crossref]
- J E Shaw, RA Sicree, PZ Zimmet, (2010) Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 87: 4-14. [Crossref]
- Y Xu, L Wang, J He (2013) Prevalence and control of diabetes in Chinese adults. JAMA 310: 948-959. [Crossref]
- S Chatterjee, K Khunti, MJ Davies (2017) Type 2 diabetes. The Lancet 389: 2239-2251. [Crossref]
- F Bragg, MV Holmes, A Iona (2017) Association between diabetes and cause-specific mortality in rural and urban areas of China. JAMA 317: 280-289. [Crossref]
- M Foretz, B Guigas, Bertrand L (2014) Metformin: from mechanisms of action to therapies. Cell Metabolism 20: 953-966. [Crossref]
- American Diabetes Association (2016) 7. Approaches to glycemic treatment. Diabetes Care, vol. 39: S52-S59. [Crossref]
- DM Nathan, JB Buse, MB Davidson (2009) Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 52: 17-30. [Crossref]
- RS Hundal, M Krssak, S Dufour (2000) Mechanism by which metformin reduces glucose production in type 2 diabetes. Diabetes 49: 2063-2069. [Crossref]
- H An, L He (2016) Current understanding of metformin effect on the control of hyperglycemia in diabetes. J Endocrinol 228: R97-R106. [Crossref]
- M Greco, E Chiefari, T Montalcini (2014) Early effects of a hypocaloric, Mediterranean diet on laboratory parameters in obese individuals. Mediators Inflamm 2014: 8. [Crossref]
- M Mensink, EE Blaak, AJ Wagenmakers, et al. (2005) Lifestyle intervention and fatty acid metabolism in glucose-intolerant subjects. Obesity Research 13: 1354-1362. [Crossref]
- LJ Goodyear, BB Kahn (1998) Exercise, glucose transport, and insulin sensitivity. Annu Rev Med 49: 235-261.[Crossref]
- VA Koivisto, H Yki Järvinen, RA DeFronzo (1986) Physical training and insulin sensitivity. Diabetes Metab Rev 4: 445-481. [Crossref]
- CO Hagan, G De Vito, CAG Boreham (2013) Exercise prescription in the treatment of type 2 diabetes mellitus: current practices, existing guidelines and future directions. Sports Med 43: 39-49. [Crossref]
- TS Church, SN Blair, S Cocreham (2010) Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: a randomized controlled trial. JAMA 304: 2253-2262. [Crossref]
- CG Sharoff, TA Hagobian, SK Malin (2010) Combining short-term metformin treatment and one bout of exercise does not increase insulin action in insulin-resistant individuals. Am J Physiol Endocrinol Metab 298: E815-E823. [Crossref]
- SK Malin, R Gerber, SR Chipkin, et al. (2012) Independent and combined effects of exercise training and metformin on insulin sensitivity in individuals with prediabetes. Diabetes Care 35: 131-136. [Crossref]
- SK Malin, J Nightingale, SE Choi, et al. (2013) Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity 21: 93-100. [Crossref]
- NG Boule, GP Kenny, J Larose, et al. (2013) Does metformin modify the effect on glycaemic control of aerobic exercise, resistance exercise or both? Diabetologia 56: 2378-2382. [Crossref]
- M Hansen, MK Palsoe, JW Helge, et al. (2015) The effect of metformin on glucose homeostasis during moderate exercise. Diabetes Care 38: 293-301. [Crossref]
- ML Erickson, JP Little, JL Gay, et al. (2017) Postmeal exercise blunts postprandial glucose excursions in people on metformin monotherapy. J Appl Physiol 123: 444-450. [Crossref]
- E. Chacko (2017) A time for exercise: the exercise window. J Appl Physiol 122: 206-209. [Crossref]
- DJ Macfarlane, CC Y Lee, EYK Ho, et al. (2007) Reliability and validity of the Chinese version of IPAQ (short, last 7 days). J Sci Med Sport 10: 45-51.[Crossref]
- H Kuipers, FT Verstappen, HA Keizer, et al. (1985) Variability of aerobic performance in the laboratory and its physiologic correlates. Int J Sports Med 6: 197-201. [Crossref]
- A Revdal, SM Hollekim Strand, CB Ingul (2016) Can time efficient exercise improve cardiometabolic risk factors in type 2 diabetes? A pilot study. J Sports Sci Med 15: 308-313. [Crossref]
- E Robinson, C Durrer, S Simtchouk (2015) Short-term high-intensity interval and moderate-intensity continuous training reduce leukocyte TLR4 in inactive adults at elevated risk of type 2 diabetes. J Appl Physiol 119: 508-516. [Crossref]
- TJ Horton, GK Grunwald, J Lavely, et al. (2006) Glucose kinetics differs between women and men, during and after exercise. J Appl Physiol 100: 1883-1894. [Crossref]
- KS Weston, U Wisloff, JS Coombes (2014) High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. Br J Sports Med 48: 1227-1234. [Crossref]
- RB Batacan Jr, MJ Duncan, VJ Dalbo, et al. (2017) Effects of high-intensity interval training on cardiometabolic health: a systematic review and meta-analysis of intervention studies. Br J Sports Med 51: 494-503.
- S Cassidy, C Thoma, D Houghton, et al. (2017) High-intensity interval training: a review of its impact on glucose control and cardiometabolic health. Diabetologia 60: 7-23. [Crossref]
- JB Gillen, JP Little, Z Punthakee, et al. (2012) Acute high-intensity interval exercise reduces the postprandial glucose response and prevalence of hyperglycaemia in patients with type 2 diabetes. Diabetes Obes Metab 14: 575-577. [Crossref]
- K Karstoft, CS Christensen, BK Pedersen, et al. (2014) The acute effects of interval- vs continuous-walking exercise on glycemic control in subjects with type 2 diabetes: a crossover, controlled study. J Clin Endocrinol Metab 99: 3334-3342. [Crossref]
- S Frontoni, P Di Bartolo, A Avogaro, et al. (2013) Glucose variability: an emerging target for the treatment of diabetes mellitus. Diabetes Res Clin Pract 102: 86-95. [Crossref]
- L Monnier, E Mas, C Ginet (2006) Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 295: 1681-1687. [Crossref]
- MR Rizzo, R Marfella, M Barbieri (2010) Relationships between daily acute glucose fluctuations and cognitive performance among aged type 2 diabetic patients. Diabetes Care 33: 2169-2174. [Crossref]
- K Torimoto, Y Okada, H Mori, et al. (2013) Relationship between fluctuations in glucose levels measured by continuous glucose monitoring and vascular endothelial dysfunction in type 2 diabetes mellitus. Cardiovascular Diabetology 12. [Crossref]
- NG Boule, C Robert, GJ Bell, et al. (2011) Metformin and exercise in type 2 diabetes: examining treatment modality interactions. Diabetes Care 34: 1469-1474. [Crossref]
- NK Gopaul, EE Anggard, AI Mallet, et al. (1995) Plasma 8-epi-PGF2α levels are elevated in individuals with non-insulin dependent diabetes mellitus. FEBS Letters 368: 225-229. [Crossref]
- JB Meigs, MG Larson, CS Fox, et al. (2007) Association of oxidative stress, insulin resistance, and diabetes risk phenotypes: the Framingham Offspring Study. Diabetes Care 30: 2529-2535. [Crossref]
- Z Radak, Z Zhao, E Koltai, et al. (2013) Oxygen consumption and usage during physical exercise: the balance between oxidative stress and ROS-dependent adaptive signalling. Antioxid Redox Signal 18: 1208-1246. [Crossref]
- SK Malin, B Braun (2016) Impact of metformin on exercise-induced metabolic adaptations to lower type 2 diabetes risk. Exerc Sport Sci Rev 44: 4-11. [Crossref]
- A McArdle, D Pattwell, A Vasilaki, et al. (2001) Contractile activity-induced oxidative stress: cellular origin and adaptive responses. Am J Physiol Cell Physiol 280: C621–C627. [Crossref]
- MJ Sampson, N Gopaul, IR Davies, et al. (2002) Plasma F2 isoprostanes: direct evidence of increased free radical damage during acute hyperglycemia in type 2 diabetes. Diabetes Care 25: 537-541. [Crossref]