Introduction: Plantar fasciitis (PF) accounts for about 80% of cases of heel pain. Foot orthoses (shoe insole/arch support), are one of the conservative management for plantar fasciitis. To our knowledge, we could not find any study that assesses the authentic benefits of using foot insoles with their different types on reducing PF pain among healthcare providers in the kingdom of Saudi Arabia (KSA). The aim of this was to evaluate the short and long-term effectiveness of foot orthosis in the recovery of plantar fasciitis and assess its influence on pain and quality of life among healthcare providers.
Methods: 93 subjects agreed to participate in the study male (n=30) 32.3%, and Female (n=63) 6.78%. All participants were asked to sign a consent form before participating in filling out the survey questions.
Study Design: Experienced Musculoskeletal researchers/Clinicians developed the study online questionnaire.
Results: 93 participants (n=30) 32.3% were male and (n=63) 64.5 % were Female. The results showed that 42 (45.2%) of the participants used the foot-orthosis and 51(45.8) did not use it. Out of the 42 participants who used the foot orthosis 33 (35.5%) benefited from the foot orthosis. A significant decrease in pain level score was reported after using the foot orthosis (3.00) compared to before using the orthosis (6.79), p= 0.000.
Conclusion: The study confirms that Planter Fasciitis is one of the common problems among healthcare providers in the KSA, and foot orthosis is one of the best conservative management for decreasing PF symptoms. the study did not find a direct effect of Age, gender, BMI, and the received PT treatments on the benefits of using foot orthosis.
Plantar Fasciitis; Heel Pain; Foot-Insole; Orthoses; Rehabilitation
Plantar fasciitis (PF) is defined as the inflammation of the thick fibrous band (Planter fascia) that runs along the bottom of the foot and is known as a common cause of heel pain in adults [1]. it is also identified as a painful condition of the foot caused by repetitive strain to the plantar fascia. Patients are classically present with severe pain in the first few steps in the morning [2]. It is recognized as one of the most common musculoskeletal complaints of the foot as it accounts for about 80% of cases of heel pain [3]. Researchers observed that 10% of the general population would experience PF at least once in their lifetime [4]. In addition, studies reported that PF is not affecting athletics alone, but it is higher in people with a sedentary lifestyle.
It has been reported that PF is not affected by age or by gender [5]. Foot and ankle pain in health care providers especially among nurses has not been well studied, as compared with other problems like low back pain or neck pain, even though foot and ankle pain can cause significant problems in daily nursing work [6]. It has been reported that shoe comfort was independently associated with foot and ankle pain outcomes. A study by Chiu et al [7]. suggested that providing comfortable footwear for clinical nurses is essential for reducing fatigue and discomfort in the lower extremities. Some studies reported that the initial treatments for plantar fasciitis are to reduce activity, minimize standing, and use anti-inflammatory drugs, foot insole, and or to use arch supports [8, 9, 10] however, If the pain continues despite all different types of conservative treatments (corticosteroid injection, shock wave, ice therapy, electro-stimulation, endoscopic plantar release, etc.), then surgery may be considered the best intervention [11]. Fortunately, it was reported that most patients respond to conservative treatment [12, 13].
It has been anticipated that one of the conservative management of plantar fasciitis was the foot orthoses (shoe insole/arch support), which reduce pain and tissue stress during standing or ambulation. There is a wide range of foot orthoses; it varies from a simple prefabricated form that can be directly used as needed and easily found in the market, to a customized form that is made according to the specific conditions of the patient’s feet. It is well-recognized that most PF patients are usually prescribed foot insoles as part of their conservative treatment [14]. Numerous studies reported that Musculoskeletal pain can cause loss of motivation to work and is known to be one of the major causes of sick leave, and early retirement and has placed a significant burden on healthcare providers, especially among nursing staff [15, 16, 17]. It has been reported that the direct cost of treating plantar fasciitis is ranging from (720 SR) 192 $ to about (1,410 SR) 376 US million dollars [18].
To our knowledge, there is no study found to assess the authentic benefits of using foot insoles with their different types and their effect on reducing PF pain among healthcare providers in the kingdom of Saudi Arabia (KSA). Therefore, it might be necessary to study the influence of foot orthoses (shoe insoles/arch support) on PF symptoms among healthcare providers at KFSHRC and to find out its actual effect on reducing pain levels, improving the quality of life, and calculating the estimated cost efficiency.
To evaluate the short- and long-term effectiveness of the foot insole/ heel cushion orthosis on the recovery of plantar fasciitis and to assess its influence on the quality of life among healthcare providers at King Faisal Specialist Hospital and Research Center (KFSHRC) and to find out its actual effect on reducing pain levels, improving the quality of life, and calculating the estimated cost efficiency.
Study design: A cross-sectional online survey research design using an online questionnaire, developed by reviewing similar existing physiotherapy surveys and consultation with experienced musculoskeletal researchers/clinicians. Descriptive statistical analysis was used to analyze the data.
Subjects: All participants were a close sample of healthcare providers working at King Faisal Specialist Hospital and Research Center (KFSH&RC), and diagnosed with plantar fasciitis.
Sample size: 93 participants male (n=30) and Female (n=63), agreed to participate in the study and completed online questionnaires.
Ethical approval: The project was approved by the Research Advisory Council of King Faisal Specialist Hospital and Research Centre in Saudi Arabia.
Consent form: All participants were asked to complete and sign a consent form that include an agreement to participate in the research study before filling out the online questionnaire. A full explanation of the study, adverse events, and the right to withdraw from the study at any time were explained.
Inclusion Criteria:
- Age group 20 – 50 years old.
- Participants diagnosed with planter fasciitis
- Male and female healthcare providers
Exclusion Criteria:
- Any foot surgery.
- History of foot fracture.
- History of any bone disease
- Diabetic foot.
- Gout disease.
- Any neurological deficit.
Outcome Measures:
A survey that has been built upon the existing updated literature review [17] was used to find out the correlation between PF and several factors such; as BMI, types of insole/heel cushion, and type of activity. In addition to the pain assessment using a Numerical Analogue Pain Scale [19] to assess the pain level before and after using the foot insole/heel cushion was used as an outcome measure for this study.
Data Collection and Statistical Analysis:
All Data were collected through an online Microsoft. Com [20] and saved in a private file, for analysis. All response data were collected, tabulated, and statistically analyzed using the” Statistical Package for the Social Sciences” (SPSS®) software for Windows® ver. [21] (SPSS Inc, Chicago, IL, USA). Wilcoxon Signed Rank Test, based on positive rank, in addition to Chi-Square Tests, were used in data analysis. All data were tested for normal distribution. Differences in demographic characteristics between participants in the sample were explored by comparing means. The significant level was set at p<0.05 and data are presented as mean and standard deviation (mean ± SD).
A total of 93 participants (n=30) 32.3% were male and (n=63) 64.5 % were Female, agreed to participate in the study and completed the questionnaires. (35.5 %) of the participant were over 50 years of age, (26.9 % ) were less than 50 years, (30.1 %) were less than 40 years, and (7.5 %) were between less than 30 years. The mean height and weight of the participants were 155.26+36.1 and 79.9+20.8 respectively and the body mass index (BMI) was 33.1+28.6 which reflects obesity remarks of BMI categories. Table 1 shows the sociodemographic characteristics of the participants.
Table 1: Sociodemographic and clinical characteristics of the participants
Demographics |
N |
(%) |
Gender Male Female |
30
63 |
(32.3)
(67.7) |
Age Group 20 – 30 31 – 40 41 – 50 >50 |
7
28
25
33 |
(7.5)
(30.1)
(26.9)
(35.5) |
Profession Physician Nurses H.C.P. |
12
37
44 |
(12.9)
(39.8)
(47.3) |
H.C.P: Health Care providers (PT, RT, Lab & x-ray tech). N: Numbers
Table 2 demonstrates that the majority of the participants (38.7%) were walking most of the day compared to 36.6% who were standing most of the day and about 24.7 % were sitting most of the time. Regarding the activity level, the current results showed that the majority (48.4%) of the participants exercising 1-2 days per week and about (21,5%) were exercising 3-4 days a week, ( 2.2%) of the participants were exercising on a daily bases, whereas (30%) of the participants were not exercising at all.
Table 2: Activity Level and Exercise Frequency
|
N |
(%) |
Activity During the day |
|
|
Sitting most of the time |
23 |
(24.7) |
Walking most of the time |
34 |
(36.6) |
Standing most of the time |
36 |
(38.7) |
Frequency of the exercise |
|
|
1 – 2/days |
45 |
(48.4) |
3 – 4/days |
20 |
(21.5) |
Never |
28 |
(30.1) |
Regarding the effect of types of shoes on plantar fasciitis, the results showed that the majority of the participants (57.0 % ) were using soft sports shoes, (22.6 %) were using flat shoes, (18.3 %) were using hard sports shoes, and (2.2 %) were using high heel shoes ( figure 1)On the other hand, regarding the effect of chronic versus acute onset of plantar fasciitis, the results of the study displayed that most of the participants (67.7%) were having the problems for more than one year, (19.4%) had the problem 3-4 weeks prior filling the survey, (4.3%) had the problem 2- 3 months, (6.45%) had it for 4-6 months, and (2.2%) had it 1-2 weeks. ( Figure 2).
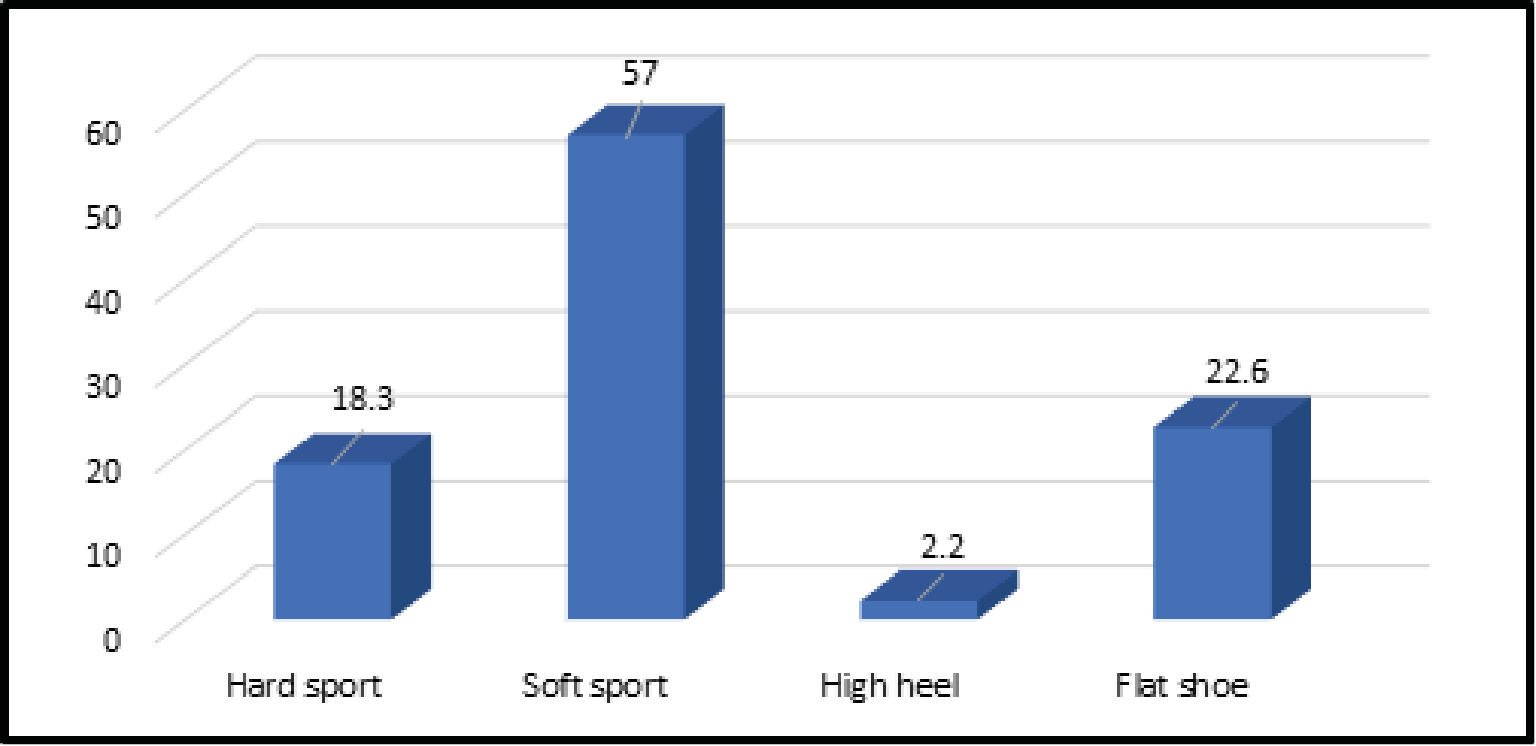
Figure 1: Percentage of types of shoes
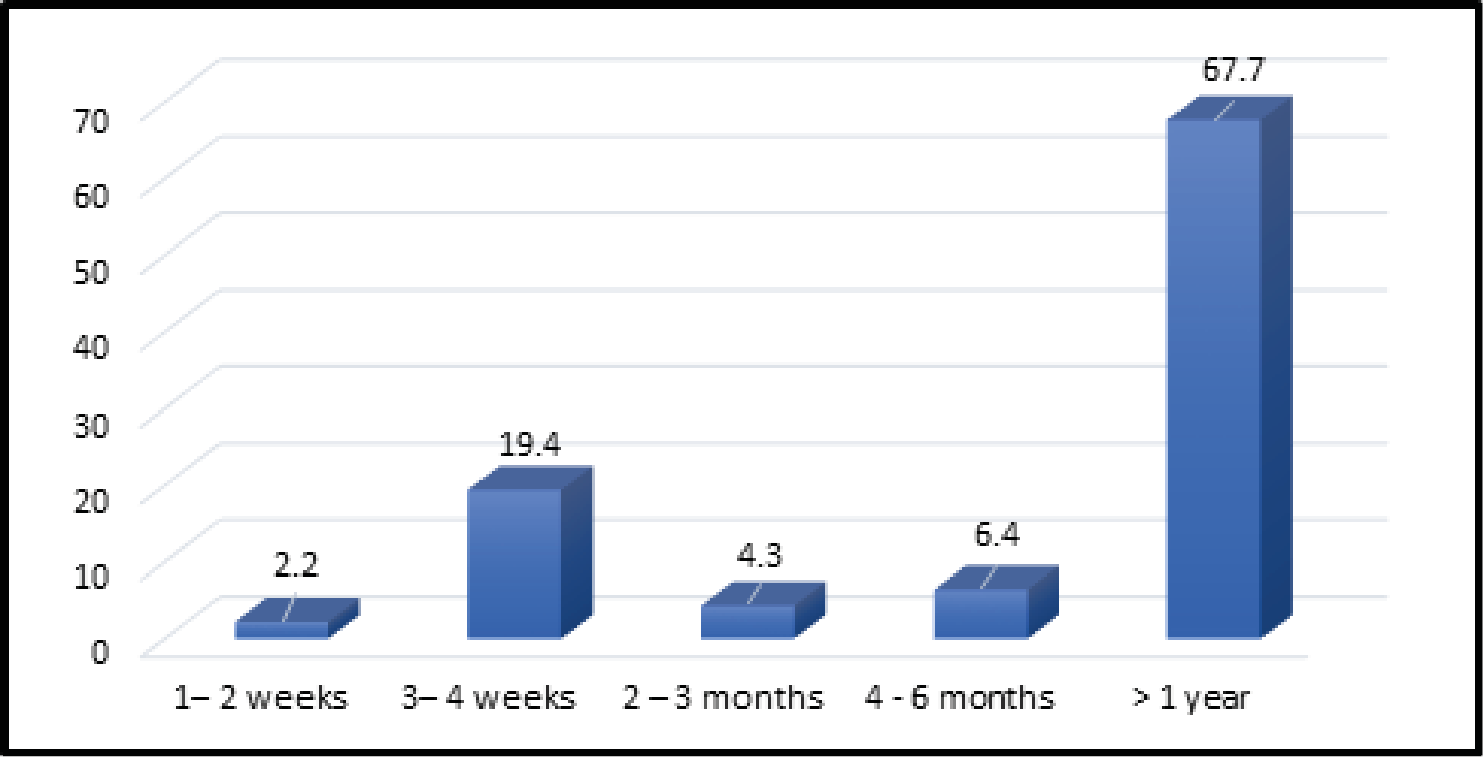
Figure 2: Percentage of onset of the PF
The results showed that 42 (45.2%) of the participants used the foot-orthosis (Insole/heel cushion) and 51(45.8) did not use it. Out of the 42 participants who used the foot orthosis 33 (35.5%) get the benefit from the foot orthosis and only 9 (9.7%) did not get the benefit. The results of the study also revealed that there was a statistically significant decrease in the pain level score for the 33 participants after using the foot orthosis pain. Almost more than 50 % improvement in the planter Fasciitis symptoms have been improved. The pain score measured by the Numerical Analogue Pain Scale [19] after using the foot orthosis was (3.00) out of 10 compared to before using the orthosis (7.00), p= 0.000.
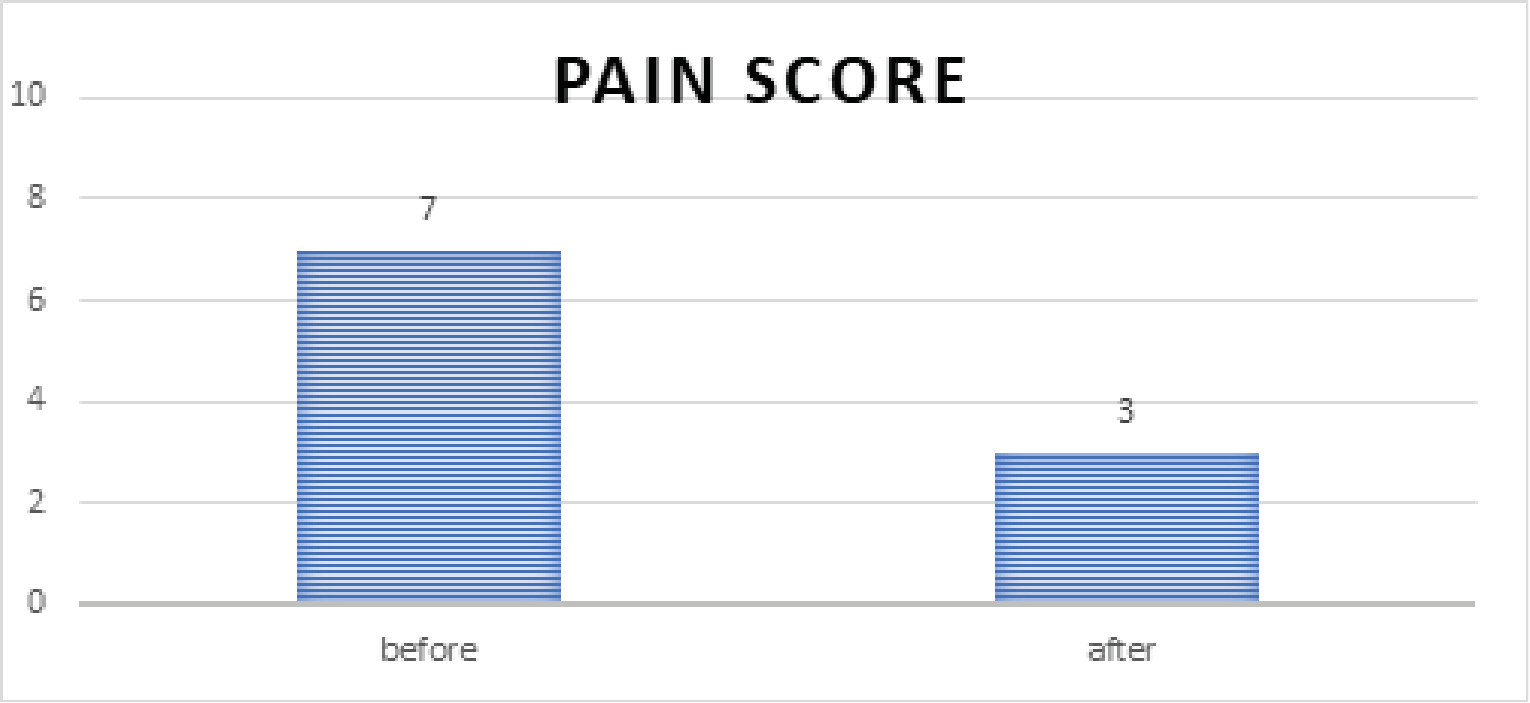
Figure 3: The pain score level before and after using the foot orthosis
In Table 3 the results showed that out of the 93 participants, only 30 (32.3%) received Physical Therapy treatments, and 63 (67.6%) did not receive them. However, by comparing the 33(35.5%) participants whose symptoms and pain improved by using the foot orthosis only 12 (85.7%) out of 14 (100%) participants receive PT treatment, whereas, 18 (94.7%) out of 19 (100%) participants did not receive PT treatments and get benefits from the foot orthosis alone, which means that the PT treatment could be clinically affecting the planter fasciitis improvement but statistically there were no significant effects p=0.091.
Table 3: Participants received PT versus benefits from foot-orthosis
|
Benefit from Foot Orthosis |
Total |
|
Yes N (%) |
No N (%) |
N % |
Received PT |
12 85.7 |
2 14.3 |
14 100% |
Did not receive PT |
18 94.7 |
1 5.3 |
19 100% |
Out of the 42 participants who used the foot orthosis, 18 (42.9%) used it for more than one year, 8(19.0%) for less than one year, 6(14.3%) used it for 4 -6 months, 5(11.9%) for 1-2 months, and finally, 5(11.9%) used it for less than one month (see figure 1). Though 52 % of the participants started using the foot orthosis after 6 months after having the planter fasciitis symptoms ( see Figure 2). But, when we compared the effect of the duration of using the foot orthosis for those who showed improvement after using the foot orthosis (n=30), the median; was 5.05(3.45, 6.15) versus those who did not improve (n=3), median; 3.36(2.32, .) respectively. The results revealed that there is no statistically significant effect for the duration on the improvement of the planter fasciitis symptoms; p =0.09.
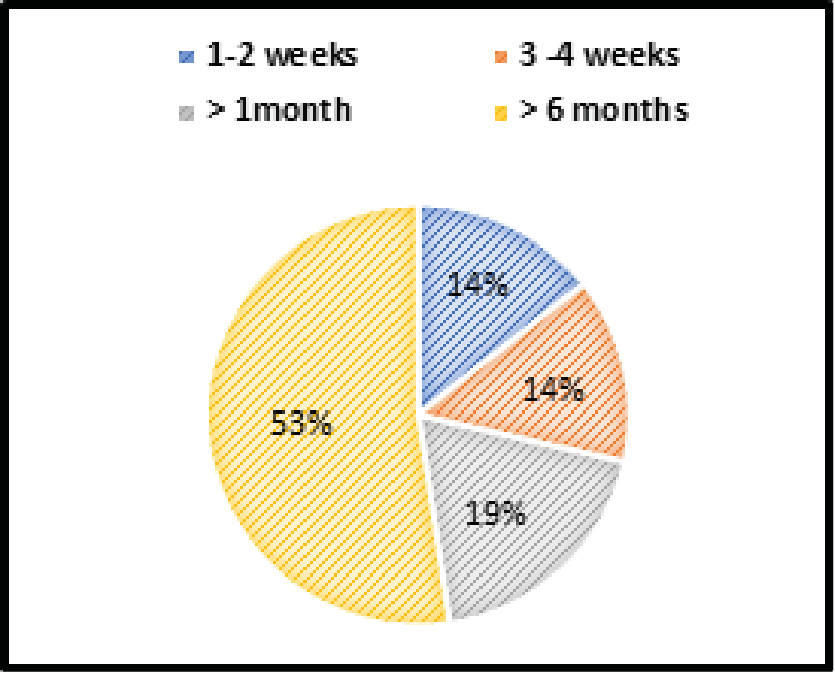
Figure 4: How early did the participants use the foot insole
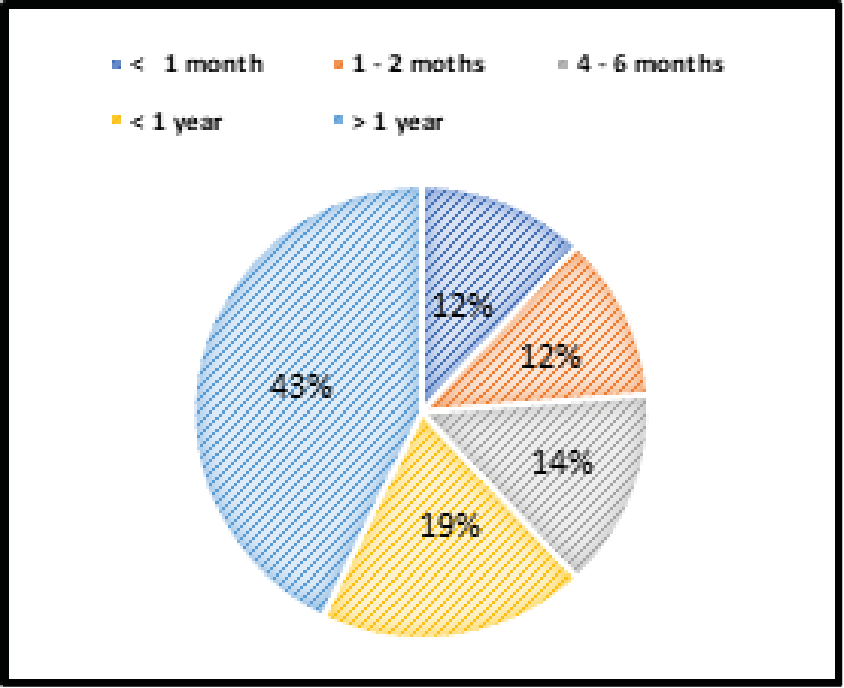
Figure 5: How long did the participants use the insole
Plantar fasciitis is one of the most common causes of heel pain in adults and one of the most common problems among healthcare providers [21]. Foot orthoses have been proven to be one of the conservative management for treating PF symptoms [14]. The aim of this was to assess the influence of foot orthoses on PF symptoms among healthcare providers at KFSHRC and to find out its actual effect on reducing pain levels, improving the quality of life, and calculating the estimated cost efficiency.
Although, there was a controversy regarding the prevalence of plantar fasciitis and whether it is more in males or females. In the current study the demographic characteristics data of the participants, The results of this study showed that the majority of the participants in this study were female (67.7%) compared to the male participants (32.3%) which may indicate that the plantar fasciitis problem is more among female healthcare providers than male. This has been testified by Moustafa et al [22]. who reported that a higher prevalence was noted in females aged 40–60 years and the female showed a worse health-related QoL for foot pain than males.
Regarding the association between gender and plantar fasciitis symptoms, the current literature showed that men and women were affected equally [23] However, some other studies showed an increased prevalence in men as reported by Taunton et al.24 who specified a significant sex difference within their study population, and showed (54%) of those affected were males and (46%) were females. While others showed an increased prevalence in women as reported by Rano et al [25]. Though, no hypothesis in the existing literature that identify the reason for the difference in the prevalence of plantar fasciitis between the two genders and is there any hormones or structural differences such as the increased incidence of anterior cruciate ligament tears in women compared with men.
Studies reported that plantar fasciitis may affect 1 in 10 people at some point during their lifetime and the most common age group is people between 40–60 years of age [24, 26]. In addition, systematic reviews reported that plantar fasciitis appears to occur most commonly between the age of 40 to 59 years [27]. In the current study (35.5% ) of the participants were over 50 years of age, (30.1%) were between 30-40, and (26.9%) were between 41-50 years of age. Therefore, about (62.4 %) of the participants, their age was between 40-60 years and which may confirm that the prevalence of PF commonly affects all ages with a higher occurrence in the age group between 40-60 years, and this coincides with the results of a study done by Crawford et al [27].
Some studies reported that Plantar fasciitis is very common in primary health care settings with obesity and a sedentary lifestyle [28] In a study done by Reb et al [29] that compared patients’ age, gender, and body mass index (BMI), they found that there was no statistical difference in the patients with different diagnoses, and they concluded that there was connectivity between the foot pathologies and the obesity. In addition, two studies done by Werner et al [30] and D’souza et al [31] did not find a significant relationship between plantar fasciitis and obesity, after evaluating numerous known risk factors related to the development of plantar fasciitis. But they confirmed the relationship between plantar fasciitis and faulty foot mechanics. Although the mean BMI of the participants in the current study was 33.1+28.6 kg/m2 which reflects obesity remarks categories, the results showed a statistically significant improvement in the planter fasciitis pain score, therefore this could confirm that there is no significant relationship between obesity and plantar fasciitis. The results of the current study corresponded with a study done by Raza et al [32] which concluded that there is no statistically significant relation between body mass index and plantar fasciitis but it could be related to foot function index and overweight. It has been reported that Physiotherapy interventions including stretching exercises, strengthening exercises, night splints, taping, dry needling, extracorporeal-shockwave therapy, and manual therapies are reported to be effective in the management of chronic plantar [33]. In addition recent studies [34, 35, 36, 37] have found Extracorporeal Shock Wave Therapy (ESWT) to be an effective modality in alleviating pain in plantar Fasciitis patients. In the current study, we did not investigate the efficacy of physiotherapy modalities(PTM), exercises, or techniques but we investigated those who received physiotherapy treatments and those who did not receive and we correlate that with the effect of that on the benefit from the foot orthosis. The results of the current study showed that there was no statistically significant correlation between those who received PTM, and the benefits from the foot insole, P=0.373, as displayed in figure 4 and 5 which showed that 94% of the participants who benefit from the foot insole, did not receive physiotherapy treatments.
It has been reported that the foot insole should be used during intermittent periods, especially in the first couple of weeks. Then the hours of using the insole should be increased gradually to reach a full day [38, 39]. Studies reported that it takes about 6-18 months to see an improvement in Plantar Fasciitis with orthotics [40, 41, 42]. The results of the current study showed that the majority of the participants (53%) who benefit from the foot-insole started to use the orthosis 6 months post the onset of PF, however, (43%) of the participants used the foot orthosis for more than one year to get the benefits and that is compatible with the previous studies reports.
The study confirms that Plantar Fasciitis is one of the common problems among healthcare providers in the KSA, and foot orthosis that known to be one of the best conservative management and has short and long-term effects on decreasing PF symptoms. Age, gender, BMI, and PT modalities were found to be clinically effective but statistically were not found to have a significant effect on the benefits gained from using the foot orthosis
Limitation of the Study
The limitation of this study is that it is a cross-sectional study in which the participants answered an online questionnaire. The lack of clinical examination and the variation in the participants’ responses may contribute to the limitation of this study. In addition, this study has been conducted in one big healthcare facility thus the results can not be generalized.
We would like to thank all the participants in the study, the Research Advisory Council of King Faisal Specialist Hospital and Research Centre, the management Team of the Physical Rehabilitation Department, the Education Team, Mr. Romeo Asuncion, Dr. Gamal Mohammed from Biostatistics Department, and Prof. Collins the Clinical Research Advisor.
All authors contributed to the concept, design, analyses, interpretation of data, drafting, and revising the manuscript critically for important intellectual content.
The authors report no conflicts of interest in this work.
- Suzan M. Attar (2012) Plantar Fasciitis: A Review Article. Saudi Journal of Internal Medicine 2.
- Riddle DL., Schappert SM (2004) The volume of Ambulatory Care Visits and Patterns of Care for Patients Diagnosed with Plantar Fasciitis: A National Study of Medical Doctors. Foot Ankle Int 25: 303-310. [Crossref]
- Van Lunen B., Cortes N., Andrus T., Walker M., Pasquale M., et al. (2011) Immediate effects of a heel-pain orthosis and an augmented low-dye taping on plantar pressure and pain in subjects with plantar fasciitis. Clin J Sport Med 21: 474-479. [Crossref]
- Gautham P., Nuhmani S., Kachanathu SJ (2014) Plantar fasciitis: A review of the literature. Saudi J Sports Med 14: 69-73.
- Davis KG., Kotowski SE (2015) Prevalence of musculoskeletal disorders for nurses in hospitals, long-term care facilities, and home health care: A comprehensive review. Hum Factors 57: 754-792. [Crossref]
- GS, Landorf KB., Menz H B (2010) Do foot orthoses change lower limb muscle activity in flat-arched feet towards a pattern observed in normal-arched feet? Clin Biomech (Bristol, Avon) 25: 728-736. [Crossref]
- Chiu MC., Wang MJ (2007) Professional footwear evaluation for clinical nurses. Appl Ergon 38: 133-141. [Crossref]
- C.Costantino., M. C. Vulpiani., D. Romiti., M. Vetrano., V. M. Saraceni (2014) Cryo-ultra-sound therapy in the treatment of chronic plantar fasciitis with heel spurs, A randomized controlled clinical study. European Journal of Physical and Rehabilitation Medicine 50: 39-47. [Crossref]
- Moyne-Bressand, S., Dhieux, C., Dousset, E., Decherchi, P (2018) Effectiveness of Foot Biomechanical Orthoses to Relieve Patients Suffering from Plantar Fasciitis : Is the Reduction of Pain Related to Change in Neural Strategy ? BioMed research international.
- H. Yu., K. Randhawa., P. Côté., C. Optima (2016) The effectiveness of physical agents for lower-limb soft tissue injuries: a systematic review. Journal of Orthopaedic and Sports PhysicalTherapy 46: 523-554. [Crossref]
- Mardani-Kivi M., Karimi Mobarakeh M., Hassanzadeh Z., Mirbolook A., Asadi K., et al. (2015) Treatment Outcomes of Corticosteroid Injection and Extracorporeal Shock Wave Therapy as Two Primary Therapeutic Methods for Acute Plantar Fasciitis: A Prospective Randomized Clinical Trial. J Foot Ankle Surg 54: 1047-1052. [Crossref]
- Goff JD., Crawford R (2011) Diagnosis and treatment of plantar fasciitis. Am Fam Physician 84: 676-682. [Crossref]
- Yucel I., Ozturan KE., Demiraran Y., Degirmenci E., Kaynak G (2010) Comparison of high-dose extracorporeal shockwave therapy and intralesional corticosteroid injection in the treatment of plantar fasciitis. J Am Podiatr Med Assoc 100: 105-110. [Crossref]
- Trotter LC., Pierrynowski MR (2008) The short-term effectiveness of full-contact custom-made foot orthoses and prefabricated shoe inserts on lower-extremity musculoskeletal pain: a randomized clinical trial. J Am Podiatr Med Assoc 98: 357-363. [Crossref]
- Lim, A. T., How, C. H., Tan, B (2016) Management of plantar fasciitis in the outpatient setting. Singapore medical journal 57: 168-171. [Crossref]
- López López D., Bouza Prego Mde L., Requeijo Constenla A., Saleta Canosa JL., Bautista Casasnovas A., et al. (2014) The impact of foot arch height on quality of life in 6-12-year-olds. Colomb Med 45:168-172. [Crossref]
- Palomo López P., Becerro de Bengoa Vallejo R., Losa-Iglesias ME., Rodríguez-Sanz D., et al. (2018) Impact of plantar fasciitis on the quality of life of male and female patients according to the Foot Health Status Questionnaire. J Pain Res 11: 875-880. [Crossref]
- Tong KB., Furia J (2010) Economic burden of plantar fasciitis treatment in the United States. Am J Orthop (Belle Mead NJ) 39: 227-231. [Crossref]
- M. P. Jensen., P. Karoly., S. Braver (1986) The measurement of clinical pain intensity: a comparison of six methods. Pain 27: 117-126. [Crossref]
- Excel for Microsoft 365, Excel for the web, Excel 202 Excel for Microsoft 365, Excel for the web, Excel 2021.
- Cotchett M., Lennecke A., Medica VG., Whittaker GA., Bonanno DR (2017) The association between pain catastrophizing and kinesiophobia with pain and function in people with plantar heel pain. Foot (Edinb) 32:8-14. [Crossref]
- Moustafa A., M. Hassanein., E. Foti., C (2015) Objective assessment of corticosteroid effect in plantar fasciitis: additional utility of ultrasound. Muscles Ligaments Tendons J. 5: 289-296. [Crossref]
- Goff JD., Crawford R (2011) Diagnosis and treatment of plantar fasciitis. Am Fam Physician 84: 676-682. [Crossref]
- Taunton JE., Ryan MB., Clement DB (2002) A retrospective case-control analysis of 2002 running injurie. Br J Sports Med.2002;36(2):95-101. [Crossref]
- Rano JA., Fallat LM., Savoy-Moore RT (2001) Correlation of heel pain with body mass index and other characteristics of heel pain. J Foot Ankle Surg 40: 351-356. [Crossref]
- Orchard.J (2012) Plantar fasciitis. BMJ 345: e6603. [Crossref]
- Crawford F., Atkins D., Edwards J (2000) Interventions for treating plantar heel pain. Cochrane Database Syst Rev CD000416. [Crossref]
- Irving DB., Cook JL., Menz HB (2006) Factors associated with chronic plantar heel pain: a systematic review. J Sci Med Sport 9: 11-22. [Crossref]
- Reb CW., Schick FA., Karanjia HN., Daniel JN (2015) High prevalence of obesity and female gender among patients with concomitant tibial posterior tendonitis and plantar fasciitis. Foot & ankle specialist 8: 364-368. [Crossref]
- Werner RA., Gell N., Hartigan A., Wiggerman N., Keyserling WM (2010) Risk factors for plantar fasciitis among assembly plant workers. Pm&r 2:110-116. [Crossref]
- D’souza JC., Franzblau A., Werner RA (2005) Review of epidemiologic studies on occupational factors and lower extremity musculoskeletal and vascular disorders and symptoms. Journal of occupational rehabilitation 15: 129-165. [Crossref]
- Raza A., Saleem S., Saeed HS., Bilal A., Zafar ZA., et al. (2021) Incidence of plantar fasciitis in overweight patients of government hospitals of Faisalabad city. Professional Med J 2021; 28: 718-724. [Crossref]
- E.M.I.A. Bandara., W.N.I. Kularathne (2019) Physical Therapy Interventions for Plantar Fasciitis: A Review Article. International Research Journal of Advanced Engineering and Science 4: 176-187.
- Ibrahim Mahmoud I (2017) Long-term results of radial extracorporeal shock wave treatment for chronic plantar fasciopathy : A prospective, randomized, placebo-controlled trial with two years follow-up. Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society 35.7: 1532-1538. [Crossref]
- Gollwitzer Hans (2015) Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. The Journal of Bone and Joint Surgery American 97: 701-708. [Crossref]
- Grecco Marcus Vinicius (2013) One-year treatment follow-up of plantar fasciitis : radial shockwaves vs. conventional physiotherapy. Clinics 68: 1089-1095. [Crossref]
- Lohrer Heinz (2010) Comparison of radial versus focused extracorporeal shock waves in plantar fasciitis using functional measures. Foot and Ankle International 31: 1-9. [Crossref]
- Pfeffer G., Bacchetti P., Deland J (1999) Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int 20: 214-221. [Crossref]
- Kogler GF., Solomonidis SE., Paul JP (1996) Biomechanics of longitudinal arch support mechanisms in foot orthoses and their effect on plantar aponeurosis strain. Clin Biomech (Bristol, Avon) 11: 243-252. [Crossref]
- Riddle DL., Pulisic M., Pidcoe P., Johnson RE (2003) Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am 85-A: 872-877. [Crossref]
- Cozta ARA., Silva HJA., Mendes AAFT., Silva RS., Lins CAA., et al. (2019). Effects of insoles adapted in flip-flop sandals in people with plantar fasciopathy: a randomized, double-blind clinical, controlled study. Clin. Rehabil, 1-11. [Crossref]
- Walther M., Kratschmer B., Verschl J., Volkering C., Altenberger S., et al. (2013) Effect of different orthotic concepts as first-line treatment of plantar fasciitis. Foot Ankle Surg, 19: 103-107. [Crossref]