This case reports saving a questionable tooth, which otherwise would have been extracted, using a hemisectioning treatment approach. A 42-years old male patient was presented with a severe pain related to the lower right quadrat. The lower right first molar had a very deep distal caries. The distal root of the tooth was removed, while the mesial root was root canal treated. A crown on the mesial half was splinted to the adjacent premolar, which had a post and core and needed a crown, making a 2-unit bridge with distal cantilevering the distal half of the molar.
An abutment molar with extensive disease may be unsuitable for restoration. In such cases, the treatment options are limited and may include a removable partial denture, fixed partial denture or a dental implant to replace the missing tooth. The term tooth resection denotes the excision and removal of any segment of the tooth or a root with or without its accompanying crown portion. Various resection procedures described are : root amputation, hemisection, radisection and bisection [1]. Alternatively, if the bone loss is limited to one root , a hemisection procedure may be possible. Periodontal, prosthodontics, and endodontic assessment for appropriate selection of cases is important. From a periodontal perspective, this procedure is indicated if there is severe bone loss limited to one root or involvement of class III furcations that could produce a stable root after hemisection. This procedure is also appropriate if the patient is unable to perform appropriate oral hygiene in the area. Extensive exposure of the roots because of dehiscence is another indication for excision of one root. From a restorative standpoint, treatment by hemisection is indicated for failure of an abutment within a fixed prosthesis, provided a portion of the tooth can be retained to act as the abutment for the prosthesis [2]. Other indications include vertical root fracture confined to a single root of a multirooted tooth or any severe destructive process that is confined to a single root, including caries, external root resorption, and trauma. The remaining root may be inoperable for the necessary root canal treatment. Also, fusion or proximity of the roots may prevent their separation [3].
Hemisection refers to sectioning of a mandibular molar into two halves followed by removal of the diseased root and its coronal portion. The retained root is endodontically treated and the furcations area is made self-cleansable by removing the lip of root carefully. Since hemisected teeth fail by root fractures, it is important to restore them adequately by an extracoronal restoration. It is indicated where one of the root of molar is unsalvageable due to caries, periodontitis, or iatrogenic mishaps . It is thus a conservative option with acceptable prognosis.
Periodontal Indications for Hemisection 1. Severe vertical bone loss involving only one root of multi-rooted teeth. 2. Through and through furcation destruction. 3. Unfavourable proximity of roots of adjacent teeth, preventing adequate hygiene maintenance in proximal areas. 4. Severe root exposure due to dehiscence [2].
Endodontic and restorative indications [4]
- Prosthetic failure of abutments within a splint: If a single or multirooted tooth is periodontally involved within a fixed bridge, instead of removing the entire bridge, if the remaining abutment support is sufficient, the root of the involved tooth is extracted.
- Endodontic failure: Hemisection is useful in cases, in which there is perforation through the floor of the pulp chamber, or pulp canal of one of the roots of an endodontically involved tooth which cannot be instrumented.
- Vertical fracture of one root: The prognosis of vertical fracture is hopeless. If vertical fracture traverses one root while the other roots are unaffected, the offending root may be amputated.
- Severe destructive process: This may occur as a result of furcation or subgingival caries, traumatic injury, and large root perforation during endodontic therapy.
Case
A 42-years old male patient was presented to the dental clinics of the college of dentistry, King Khalid University with a severe spontaneous and continuous pain related to the lower right quadrant. The patient has a controlled asthma and has had several teeth restored and extracted previously with no noticeable complications.
Upon examination the lower right first molar (46) had a very deep distal caries. The distal margin was too deep and there was a gingival overgrowth onto the distal cavity. The tooth was tender to vertical percussion. It was diagnosed as symptomatic irreversible pulpitis with symptomatic apical periodontitis (Figure 1).

Figure 1. Pre-operative view (A) and X-ray (B) of lower right first molar (the white line is an artifact).
Treatment Plane
The treatment alternatives were either a crown lengthening to expose the distal margin or extract the distal half of the tooth (hemisectioning). The crown lengthening would result in deep distal cervical embrasure that is difficult to clean, thus the hemisectioning approach was chosen. This was planned to be followed by root canal treating the mesial root then place a post to help retains the crown. Anesthesia start with LIDOCAINE 2% followed by rubber dam isolation, root canal treat start with K file size 6 , 8,10 & 15 sequentially working length MB 18 mm & ML 18 mm then complete treatment by rotary PROTAPER system with irrigation using Sodium hypochloride 5.25 % [5,6] & EDTA 17% to remove smear layer one minute [7] then obturation don with gutta percha, after that build up the cavity with packable composit ( 3M filtek Z350 ) extraction done for distal root (Figure 2)
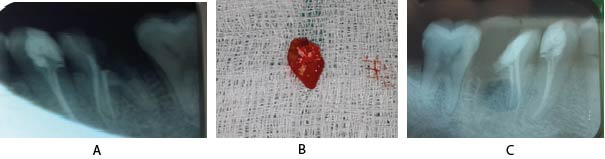
Figure 2. (A) RCT for the mesial root, (B) The extracted distal root and (C) A post-operative X-Ray
Follow up with patient for healing two months with no symptoms. Further, the adjacent premolar (45) was planned for a root canal treatment, post and a crown. Thus, it was decided to splint the two crowns to strengthen them. The occlusal scheme was designed to prevent the initial contact on the distal cantilever, which is a major drawback of the bridge design.
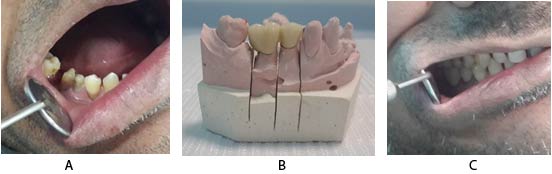
Figure 3. (A) Prepared teeth (45 & 46), (B) The fabricated 2-unit bridge and (C) The bridge after cementation.
Preparation done final impression done with PVS material for a 2-unit bridge ceramometal was fabricated, metal try-in done and shade selection .
Final cementation done with resin cement. This was followed-up for a period of 2 months.
Objectives of Hemisection [4]
- To facilitate maintenance
- To prevent further attachment loss
- To obliterate furcation defects as a periodontal maintenance problem.
Contraindication [2]
a. Strong adjacent teeth available for bridge abutments asalternatives to hemisection.
b. Inoperable canals in root to be retained.
c. Root fusion-making separation impossible.
Periodontal, prosthodontics, and endodontic assessment for appropriate selection of cases is important. Buhler stated that hemisection should be considered before every molar extraction [8], because it provides a good, absolute, and biological cost saving alternative with good long term success. The treatment options to replace severely damaged and possibly unrestorable teeth include removable partial denture, fixed partial denture, and dental implant. A guiding principle should be to try and maintain what is present [9]. The use of hemisection to retain a compromised tooth offers a prognosis comparable to any other tooth with endodontic treatment . Treatment by crown lengthening has disadvantage like Bad oral hygiene, Existing Periodontitis & Inadequate attached gingival .
Periodontic Phase
Endodontic treatment was performed first but in this case there is more soft tissue in coronal portion we can't do endo treatment so, we did gingivactomy first & follow up.
Endodontic Phase
Follow up 2 weeks after gingivectomy then Endodontic treatment was performed , if the tooth could not be treated endodontically or if there was an endodontic failure, the case would be contraindicated for hemisection .
LIDOCAINE 2% followed by rubber dam isolation, root canal treat start with K file size 6 , 8,10 & 15 sequentially working length MB 18 mm & ML 18 mm then complete treatment by rotary PROTAPER system with irrigation using Sodium hypochloride 5.25 % [5,6] & EDTA 17% to remove smear layer one minute [7] then obturation don with gutta percha .
Periodontic Phase
We do first post in endodontic treatment in secondary premolar Four critical factors in selecting molar for hemisection are following ;
(1) Root Divergence. Ideally the resected root should have generous root divergence, as close root proximity will make surgery difficult. (2) Root Form. Roots of mandibular molars show concavity, mostly on distal root. Therefore, odontoplasty should be performed to provide a proper contour. (3) Location of Furcation. Closer the furcation opening to the cemento-enamel junction, better the prognosis for retained root. (4) Remaining Root Attachment. is critical to evaluate; as cylindrical, ovoid, and long root serves as an excellent abutment.
Objectives (1) To facilitate maintenance. (2) To prevent further attachment loss. (3) To obliterate furcation defects as a periodontal maintenance problem.
Prosthodontic Phase
When the tooth lose part of its root support, it will require a restoration to permit it to function independently or serve as an abutment for fixed partial denture or splint. Thus, restoration is required for function and stabilization of occlusion.
Points to consider while fabricating the prosthesis: Restoration can contribute to periodontal destruction, if margins are defective or if nonocclusal surfaces do not have physiologic form. An improperly shaped occlusal contact area converts acceptable forces into destructive forces leading to ultimate failure of hemisection. Hemisected abutment are given a taper greater than 6–10 degree to have a path of insertion compatible with the anterior abutment and to compensate for this buccal and lingual grooves are placed in the abutment. Occlusal table is reduced in size in order to decrease the forces on the retained hemisected root. Cuspal inclines are made less steep to reduce laterally directed forces and eliminate the nonworking contacts. Retained root is restored as premolar which helped to reduce the masticatory load. Stein noted that “esthetic permitting, the sanitary pontic is the best design for posterior region” .
The keys to long term success include thorough diagnosis, selection of patients with good oral hygiene, careful surgical and restorative management. Hemisection may be a suitable alternative to extraction and implant therapy and should be discussed with patients during consideration of treatment options [2].
Considering the limitation of this report, tooth hemisectioning seemed to be a viable alternative to extracting questionable teeth. Case selection is of paramount importance to the success of this treatment modality.
This report was supported by the college of dentistry, King Khalid University and has never been presented elsewhere.
- Parmar G, Vashi P (2003) Hemisection: a case-report and review. Endodontology 15: 26-29. [Crossref]
- Jain A, Bahuguna R, Agarwal V (2011) Hemisection as an Alternative Treatment for Resorbed Multirooted Tooth-A Case Report. Asian Journal of Oral Health & Allied Sciences 1(1): 44-46. [Crossref]
- Park J (2009) Hemisection of teeth with questionable prognosis. Report of a case with seven-year results. Journal of the International Academy of Periodontology 11(3): 214-219. [Crossref]
- Arora A, Arya A, Singhal RK, Khatana R (2017) Hemisection: A conservative approach. Indian J Dent Sci 9: 206-209. [Crossref]
- Farzaneh S, Parirokh M , Nakhaee N, P. V. Abbott PV (2018) Effect of two different concentrations of sodium hypochlorite on postoperative pain following single-visit root canal treatment: a triple-blind randomized clinical trial. Int Endod J. [Crossref]
- Calt S1, Serper A (2002) Time-dependent effects of EDTA on dentin structures. Endod 28(1): 17-9. [Crossref]
- Alamoudi R (2019) The smear layer in endodontic: To keep or remove – an updated overview . [Crossref]
- Newell DH (1998) The diagnosis and treatment of molar furcation invasions. Dent Clin North Am 42(2): 301-337. [Crossref]
- Weine FS, Smulson MH, Herschman JB (1996) Endodontic therapy. 5th Ed ed. St. Louis: Mosby 640-641.